
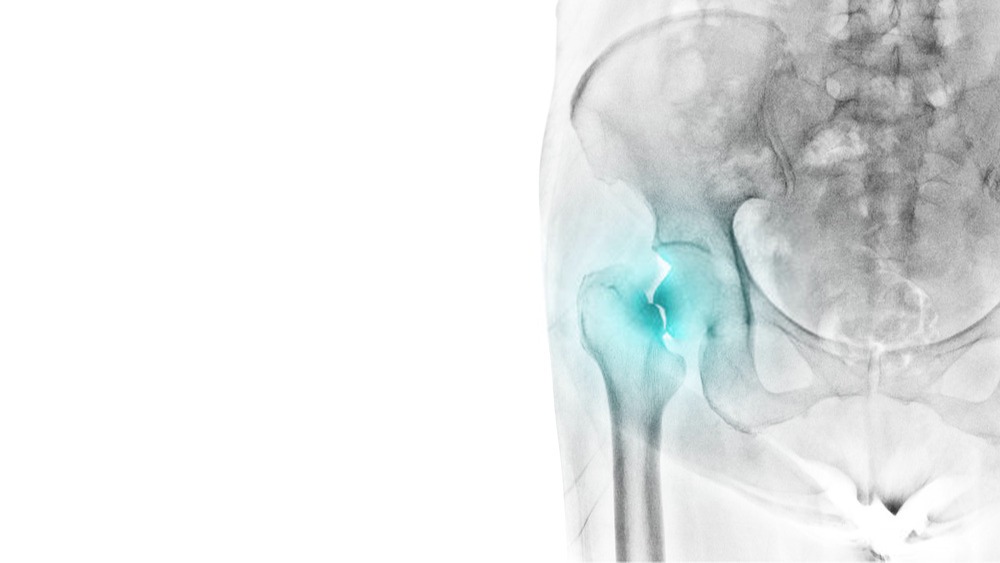
A femoral neck fracture is one of the most common fracture in the lower limb. In younger patients, it is usually an outcome of a high energy trauma (e.g. road traffic accidents) while in older patients femoral neck may fracture spontaneously due to senile osteoporosis. This article will focus on the rehabilitation for femoral neck fractures highlighting the objectives of rehabilitation, anticipated bone healing and rehabilitation duration and special considerations for rehabilitation including gait, weight bearing and return to functional activities.
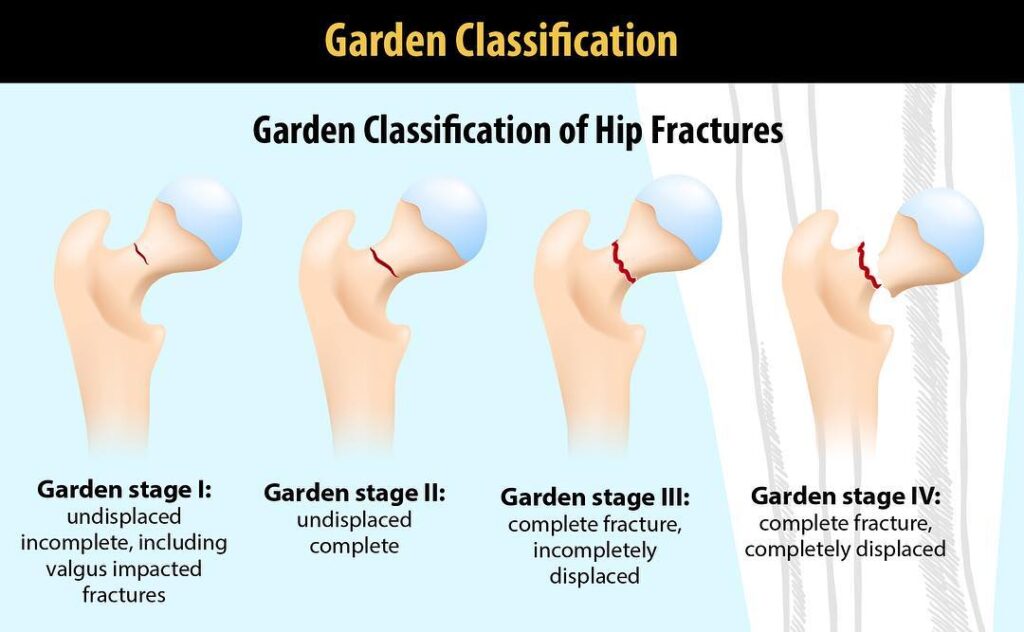
Classification of Fractures: The femoral neck fractures are classified using the Garden’s classification criteria. Garden’s I is an incomplete impacted femoral neck fracture whilst Garden’s type II is a completed though non-displaced femoral fracture. A displaced fracture which may be accompanied by disruption of joint capsule is classified as Garden’s III whilst a completely displaced femoral neck fracture is classified as Garden’s type IV. This usually has poorest prognosis and may lead to avascular necrosis of the femoral head. Figure below depicts the four levels of femoral neck fractures.
Orthopedic Objectives: As with any fracture, the key objectives of orthopedic intervention are to restore alignment and achieve stability if the fracture is displaced or maintain alignment in non-displaced fractures. Satisfactory alignment after reduction of an unstable fracture should have no more than 15 degrees of valgus and 10 degrees of anterior posterior angulation.
These fractures have a high rate of non-union and avascular necrosis because of disruption of blood supply to femoral head.
Rehabilitation Objectives: The key goals for rehabilitation of femoral neck fractures and physiotherapy intervention are to restore the range of motion at hip and knee and to improve strength in lower limb muscles. The primary muscles affected are: Gluetus medius, iliopsoas, gluteus maximus, adductor magnus, longus and brevis. In addition due to exposure during surgery, quadriceps and hamstrings may also be affected. Functional recovery may focus on gait retraining and return to work and play.
Recovery and rehabilitation: Patients with impacted and rigidly fixed fractures may be able to walk with partial weight bearing within the first week though unstable or comminuted fractures are generally non weight bearing. Initially passive range of motion is initiated as active ROM is quite painful. However as pain and swelling subside within a few days, active range of motion is instituted. As vastus lateralis is exposed during surgery, keen extension may also be painful. Active ROM of knee and ankle is encouraged.
For strengthening, gluteal muscles and quadriceps is needed to enhance muscle strength. Patient may need support with transfers and dressing in the initial stages. Between 12-16 weeks, patients should usually be weight bearing as tolerated with use of assistive devices such as crutches as needed, range of motion should be within normal range, regaining muscle strength and emphasis should be on normal gait.
Timescales: The expected duration of fracture healing is 12 -16 weeks whilst rehabilitation duration may vary from 15-30 weeks.
Complications: Some of the complications of fracture neck of femur include avascular necrosis of head which may require prosthetic replacement. Other issues may be non-union, leg length discrepancy as well as prominent and painful screws, pins and plates. These may need to be removed.
Case Management Considerations: As a case manager, it is vital to understand the routine fracture healing process as well as specific considerations for fracture neck of femur. Gradual progression of weight bearing, strengthening and gait retraining along with support required in the earlier stage of recovery are aspects to be considered in rehabilitation planning.
As the patient regains strength focus will then shift to functional activities and return to work.